OrthoATITM Summary of clinical evidence
Innovative treatment for chronic tendon injuries
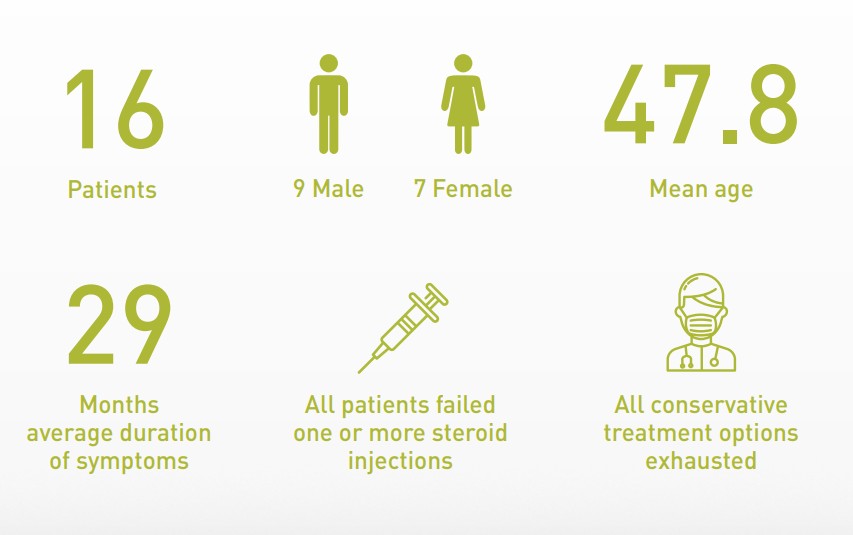
Long term data in tennis elbow (lateral epicondylitis)1.
Lateral epicondylitis (LE) is the most commonly diagnosed condition of the elbow. It occurs mostly in patients whose activities require strong gripping or repetitive wrist movements. Although LE generally resolves within 6 months, approximately 10% of patients continue to experience persistent pain and loss of function after 6 months of conservative treatment.2 . This results in significant disability, health care use, lost productivity and financial cost.
1
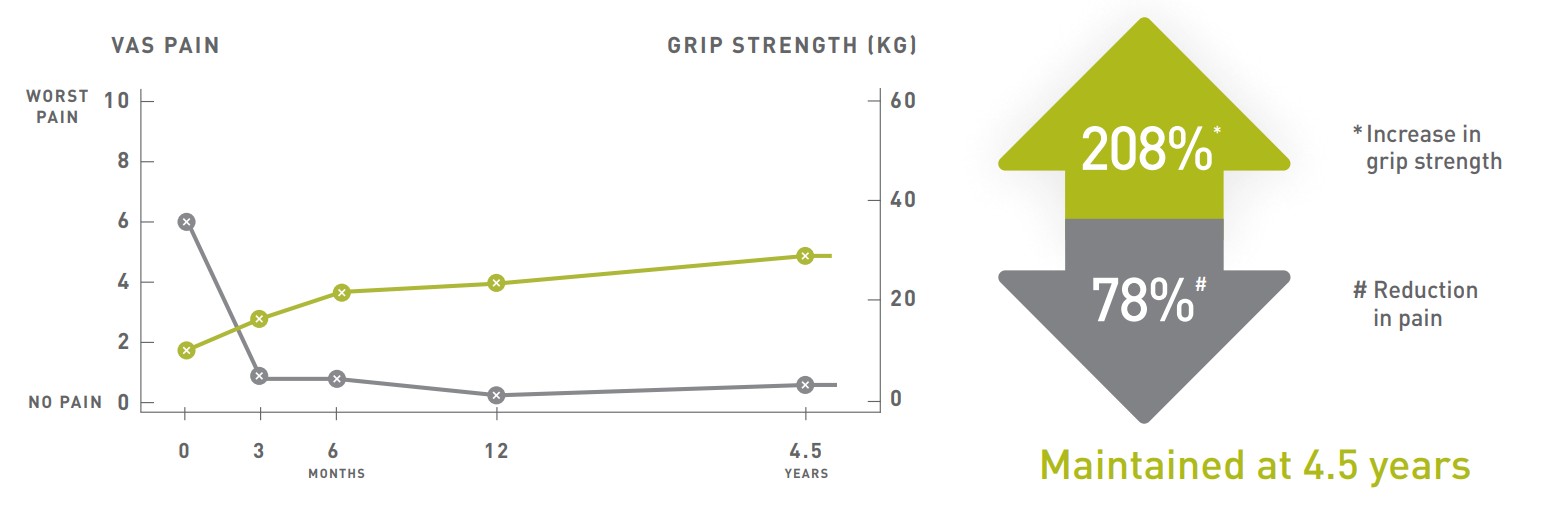
Treatment of
OrthoATI™
resulted in:
1. Evidence for the Durability of Autologous Tenocyte Injection for Treatment of Chronic Resistant Lateral Epicondylitis – Mean 4.5-Year Clinical Follow-up Am J Sports Med. 2015 Jul;43(7):1775-83.
2. The Epidemiology and Health Care Burden of Tennis Elbow: A Population-Based Study. Sanders et al. Am J Sports Med. 2015 May;43(5):1066-71.
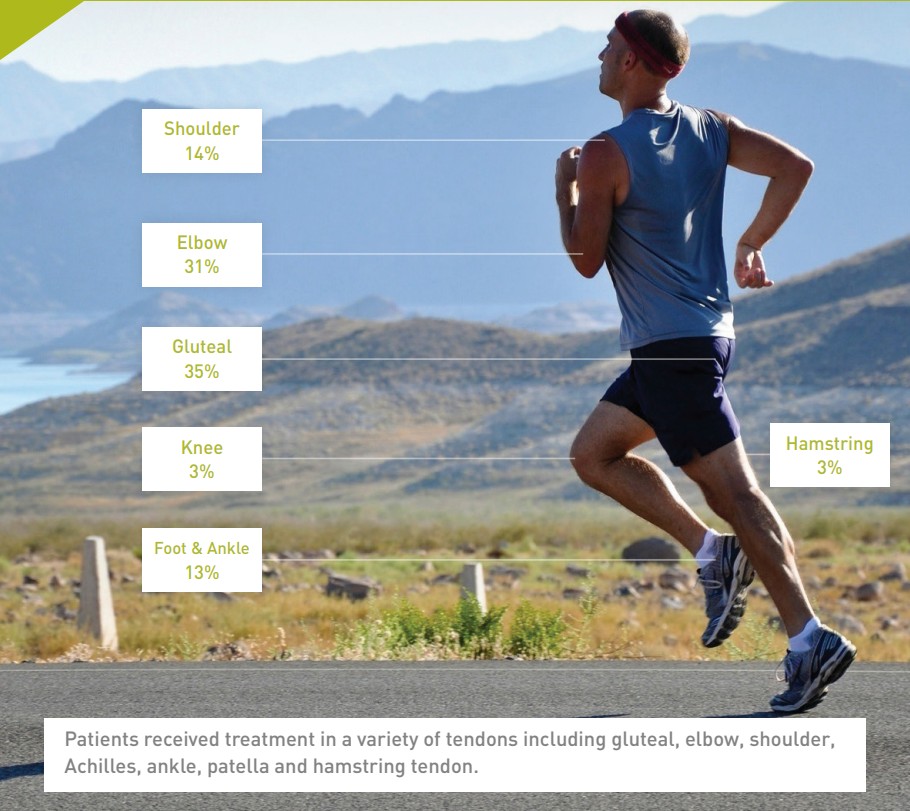
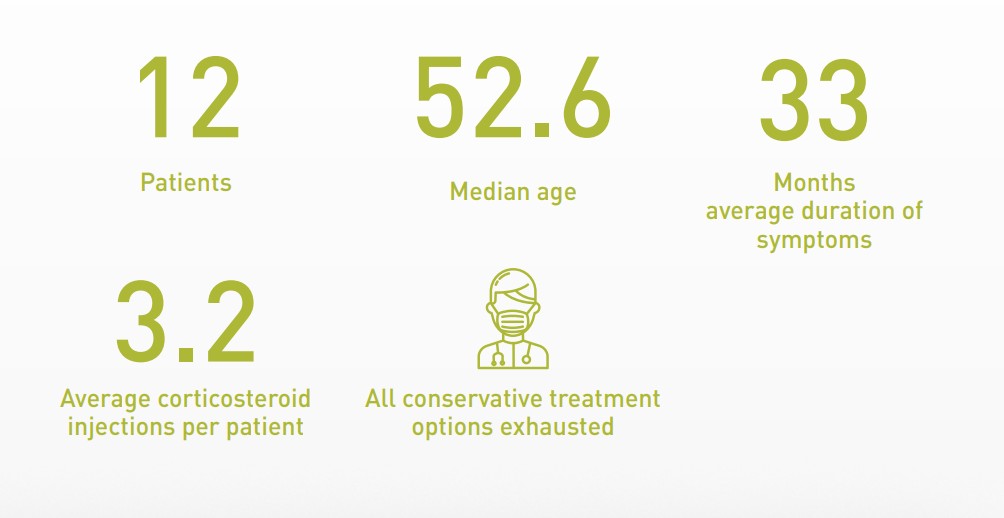
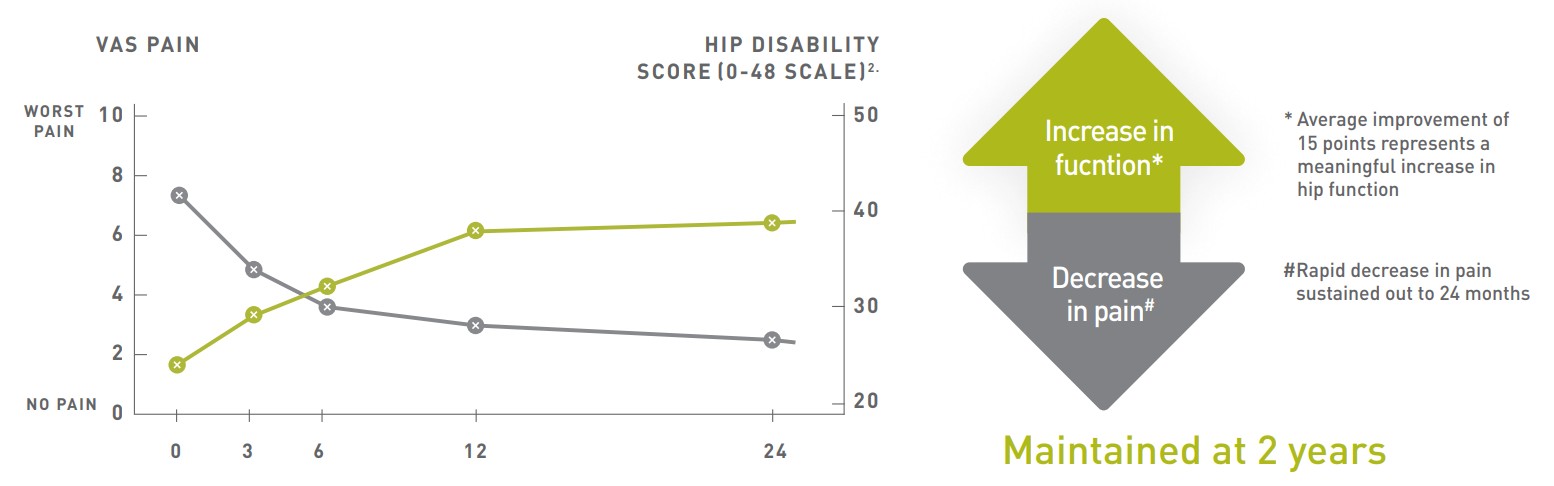
Long term data for gluteal tendinopathy.1.
Gluteal tendinopathy is a common cause of lateral hip pain and is frequently described as a constant ache on the side of the hip. Pain is often at its worst in the morning, leaving patients unable to perform their normal daily activities. Recurring symptoms are common after standard conservative treatments.
1
Treatment of
OrthoATI™
resulted in:
1. Autologous Tenocyte Injection for the Treatment of Chronic Recalcitrant Gluteal Tendinopathy – A Prospective Pilot Study Orthop J Sports Med. 2017 Feb 21;5(2):2325967116688866.
2. Oxford Hip Score – Questionnaire on the perceptions of patients about total hip replacement. J. Bone Joint Surg Br. 1996 Sep, 78(5):856
Workers compensation data1.
Tennis elbow (lateral epicondylitis) is painful, difficult to treat and has a long period of recovery. It is a common workrelated injury that may require extended periods of sick leave or restricted duties.
OrthoATITM was used to treat a group of patients (n=24) with long-term symptoms of tennis elbow (average of 2 years) and who failed to respond to other treatments.
Patients who needed time off work due to their injury missed an average of 141 days. When they did return to work, patients had restricted duties or reduced hours
“Before having the treatment I underwent three lots of surgery and had pretty much accepted I would never be 100% again. I have experienced a 100% recovery, I am pain free, able to exercise and run without issue. I have been able to continue my job as a tactical flight officer.”
Dean Allison
24
Patients

14 Male 10 Female
46
Median age
23.7
Months average duration of symptoms
78%
Of patients had multiple treatments with an average of 3 treatments per patient
After a single OrthoATITM treatment:
88%
Of patients were able to return to work within 1-3 months of treatment
70%
Of patients were able to return to work with no restrictions to their duties
75%
0f the patients who were manual labourers were able to return to work without restriction
1. Autologous Tenocyte Injection (ATI) for the Treatment of Compensating Occupationally Related Lateral Epicondylitis – A Retrospective Case Study (Presented at TOBI congress 2018)
Annual quality survey data1.
The annual quality survey (AQS) has been administered four times between 2016 and 2020 with one hundred and sixty patients responding. The AQS evaluates patient satisfaction with their treatment.
Results across all treatment areas:
73%
Of patients were satisfied with how OrthoATI™ treatment improved their symptoms
81%
Of patients did not receive any further medical treatment for their tendon injury
94%
Of patients did not require surgical intervention to relieve symptoms
1. Orthocell Annual Quality Survey 2016 – 2020
“Prior to OrthoATI™ I had corticosteroid injections, blood/PRP injections and three separate surgeries and nothing worked. I could not walk 2kms without severe swelling and pain. I was in constant pain every night and for three years I woke at 3am in severe pain. Four weeks after the injection I walked 12km’s, slept soundly and exercised without a limp. I can also run again”.
Jane Naughton